
The massive opportunity in women's longevity
This edition of Second Opinion is sponsored by:
Seraphina Therapeutics is a health and wellness company dedicated to improving global health by discovering and developing essential fatty acid therapeutics to slow aging, extend wellness, and prevent, manage, and treat chronic diseases.
Written by Leslie Schrock
The quest to defy death makes splashy headlines for extremes like billionaire blood boys and Brian Johnson’s $2M annual body optimization budget. Most of the longevity market is focused on men, whose bodies are simpler to manage and change. Women are not small men, and our differences—from body composition, hormones, reproductive system, and metabolism, to name a few—require a more nuanced approach. In this nascent market, what this approach should be depends on who you ask.
As a long-time biohacker, 2x author, and research nerd approaching perimenopause, I am obsessed with this topic, so much so that it will likely be a third book. While writing this piece, I spoke to menopause specialists, longevity researchers and enthusiasts, and founders. I also included a few notes about my own longevity journey in italicized sections below.
So here is what I learned about the female longevity market and opportunity. Tl;dr: It’s untapped and massive.
State of the women’s longevity market
The closest we have to a mainstream longevity industry in women’s health is the exploding menopause market. Thanks partly to stories (and startups) from celebrities like Naomi Watts, Gwenyth Paltrow, and Halle Berry, menopause got a serious glow-up in the public eye, and women are finally learning about this life transition. The average age of menopause hasn’t changed—it’s still 51—but cultural representations of the 40s and 50s look nothing like they did a few decades ago. Women are actively looking for ways—aesthetic and otherwise—to extend youth longer than ever before.

In general, the conversation around female longevity and any form of public experimentation is scant relative to men, and no Huberman, Attia, or Johnson-like figure owns that market and is broadening the scope beyond menopause. That’s a shame. Women over 50 have $15 trillion in spending power and control 95% of their household’s purchasing decisions.
The menopause market is projected to hit $27B by 2033. But right now, women still pay more to look good than to feel good. The injectables market—which includes Botox and fillers—is set to hit $40B by 2034, and its growth is largely driven by the expanding pool of women over 50. There is a growing ecosystem of exclusively menopause-focused startups working to fill their needs, and Midi, EverNow, and Alloy alone have collectively raised north of $150M. Right now, most are treating acute menopause symptoms with HRTs, GLP-1s, supplements, lubes, creams, and devices promising vaginal rejuvenation or aesthetic improvements.
Considering how underserved and desperate menopausal women are, this is a huge and necessary leap forward. But, in my opinion, it’s not enough, and we’re starting too late. Without a truly integrated care model that starts before menopause, the opportunity to add high-quality years to women’s lifespans is missed. And by not getting ahead of symptoms before we know they will start, we’re inflicting unnecessary suffering on women, too.
Americans are falling further behind the rest of the world in life expectancy, and the years women are expected to live in good health are projected to decline by 2050. For men, aging is more gradual, and maintenance in the 40s and beyond is mostly about muscle mass, testosterone levels, and cardiovascular health. For women, menopause is the moment when hormone levels dramatically shift, and health risks related to cardiovascular, bone, and mental health rise.
To offer a personal example, I started to struggle with sleep at 40. That’s not uncommon, but after enough nights of horrible sleep quality after even a single cocktail, I reduced my alcohol intake significantly. I wasn’t drinking much anyway with two young kids, and I’m not a teetotaler—if I want a cocktail or glass of wine, I have it. But now, it really has to feel worth it.
The curse of our aging ovaries
The root cause of hormonal changes and menopausal symptoms in women is ovarian aging. The ovaries age 2.5x faster than the rest of the body’s organ systems; we don’t know why. Their decline is tied to decreased neurocognitive, cardiovascular, immune, and bone health. Humans are in a tiny group of mammals—orcas, three species of toothed whales, and a small community of chimpanzees in Uganda—that go through menopause. For all others, life ceases shortly after the reproductive years conclude.
There are many evolutionary theories around menopause, but no one has proven yet that menopause is a biological imperative for humans. Increasing the ovaries' shelf life and eradicating the menopausal transition might just be the holy therapeutic grail. Companies like Gameto (where I am on the bioethics board), Oviva, and Celmatix are working on different approaches, and we’re creeping closer to human trials—but these drugs aren’t there yet. In the meantime, the rate of aging is not entirely tied to the ovaries, and improving other biomarkers can make a meaningful difference until they are.
Biological age vs. chronological age
Aging is not a single process or linear; the most substantial changes to the immune system and metabolism for men and women happen at 44 and 60. Those planning to live until 200 may be disappointed to hear that radical life extension was deemed implausible with today’s technologies. Since 1990, improvements in life expectancy have decelerated. The human lifespan has a hard cap at 125 years, and surviving to age 100 is unlikely to exceed 15% for women and 5% for men—for now, anyway.
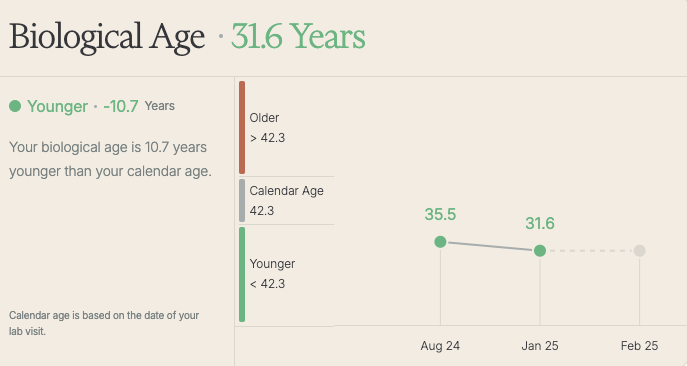
We measure age chronologically, the number you mark each year on your birthday, and biologically, or how quickly your body is aging based on DNA methylation patterns and other biomarkers. Chronological age marches on no matter what you do; biological age can be +/- chronological and improved.
I tried Function and learned that, at least by their calculations (see graphic below), my personal longevity project is working. My first blood draw in August followed a long case of COVID-19. Nothing meaningful in my routine changed before the second draw, so the state of the immune system must be a major data point. My 2025 challenge is to reduce my biological age even further.
So, what’s my longevity recipe? I am a fan of the 80/20 approach (80% of the time, I adhere; 20% of the time, I don’t, but in moderation). I eat whole, unprocessed foods cooked at home as often as possible (Mediterranean-style) on a 16:8 intermittent fasting schedule (eating between 10-6 pm) most days. Like Steve Jobs wearing a black turtleneck every day, my diet is boring and repetitive but not without the occasional pain au chocolat. My supplement stack is minimalist: magnesium, Novos Core, a multivitamin, and a new addition, pentadecanoic acid via Fatty15, which, according to my EightSleep, has positively impacted my deep sleep over the past 2 months.
Lifestyle factors that most impact women’s longevity
A large study identified lifestyle factors that cause a 13% reduction in mortality, and 40-year-old men or women who adopt all of them could add up to 24 years of life.
They are:
Positive social relationships
Good sleep hygiene
No binge drinking
Moderate diet
Minimal stress
No smoking
No opioid use disorder
Regular physical activity
But remember the caveat? These lifestyle changes must start by 40 to have the intended effect; menopause is too late. But we don’t have enough providers trained to give this advice. Every woman who lives past 50 will go through menopause, yet there is only one menopause specialist for every 32,000 American women. Ob-gyn training in the early 2000s was primarily obstetrics-focused; there was little to nothing about menopause. Dr. Shannon Cothran, a gynecologist specializing in menopause care and the founder of Meno-Start, mentioned one reason for the lack of training is that most older women have Medicare and don’t come to resident clinics for care.
Women are getting some of this information (and a slew of misinformation) from influencers. However, everyone in this age cohort should see a specialist in person or via telehealth for a more personalized plan. Dr. Jessica Kassis, a menopause provider in the Bay Area, says that in her practice, “I preemptively discuss possible perimenopausal symptoms quite early, typically in the mid-30s. During perimenopause, we will address it again as symptoms arise, which they almost always do.“
The power of movement
If exercise were a drug, everyone would have a prescription—especially women in midlife. Women who exercise reduce their risk of a fatal cardiovascular event by 36% and significantly reduce their all-cause mortality. However, only around a third of women meet weekly aerobic exercise recommendations—2-2.5 hours of moderate-intensity exercise or 1.25-2.5 of vigorous exercise each week with two or more days of strength-based activities. Only 20% of women do any strength training.

Dr. Nisha Patel, an obesity medicine physician focusing on women, tells her patients not to underestimate the importance of building muscle for long-term health and preventing frailty as we age. “Aerobic exercise is important too, but resistance training is often forgotten.”
Roma van der Walt, the founder of Vitelle, a health intelligence platform for women 35+, cautioned, “The importance of strength training is undeniable. However, we observe cohorts of women who think Pilates is sufficient, but it doesn’t load the muscle with enough weight to stimulate muscle growth. The demonization of cardio has led to women avoiding it because it is classified as muscle-damaging and ineffective. VO2 max is an important marker of longevity, and zone 2 training promotes recovery from other training and teaches the body to efficiently switch from carbohydrate to fat burning, positively affecting insulin sensitivity, possibly preventing type 2 diabetes.”
Long known to elite athletes, VO2 max is now recognized as perhaps the best single marker of longevity. The score tells you how well your body metabolizes oxygen and is a key indicator of cardiovascular fitness. A high VO2 max is associated with a lower risk of death from all causes. Lab-based tests are still the gold standard for measuring VO2 max but are not cheap. Apple, Garmin, Whoop, Oura, and other wearables makers let you measure through heart rate and GPS data, so accessing this data point is easier than ever before.
I spent most of my 20s running, then switched to CrossFit-style strength training in my 30s. I even did CrossFit through my first pregnancy (with many modifications). But, post-two kids, my pelvic floor needed work, so I took up pilates, which I love for its targeting of tiny forgotten muscles. Now at 42, it’s pilates, weight and resistance training, and a dash of cardio as brisk walks (easy as a New Yorker) and long, slow jogs. Workouts are sometimes just 20-25 minutes at home when time is tight, but I try to do something 3-4 days per week. My VO2 max is high even on this plan.