
As part of my new Second Opinion authors program, I invited Ann-Somers Hogg, director for health care at the Clayton Christensen Institute, to write about labor staffing and burnout issues. Her inaugural column tackles the question of whether we should be moving to four-day work weeks. As always, we’d love to hear your thoughts!

By Ann-Somers Hogg
You are probably tired of hearing that physicians suffer from high levels of burnout. But it remains a topic of industry conversation because it is both an egregious problem that touches every corner of the healthcare ecosystem, and because no one has figured out the solution yet.
We need a new approach to solving burnout at scale, and it will entail a systemic shift. For a health care system as entrenched, complex, and complicated as ours here in the U.S., that’s no small undertaking. But the status quo is ineffective and unacceptable.
Some innovators are starting to move the needle within their organizations, which I view as promising. One approach gaining popularity across health systems involves significantly increasing providers’ workplace flexibility. Before you decide that’s impossible, read on to see how we just might make it work!
The state of physician burnout
To solve the problem of burnout, we must understand its scale. After peaking in 2021 at almost 63%, the American Medical Association (AMA) and Medscape both report that in 2024, physician burnout is finally back below 50%—barely. That means roughly half of the physician population in our country is suffering from burnout, which the WHO describes as, “resulting from chronic workplace stress that has not been successfully managed.”
Diving into the results of Medscape’s most recent survey, 56% of female physicians reported burn out, compared to 44% of male physicians.This gender-based difference is consistent for employees broadly, with more female employees reporting burnout than their male counterparts. Most respondents indicated feelings of burnout had been experienced for over a year, with 42% reporting burnout had lasted over two years.
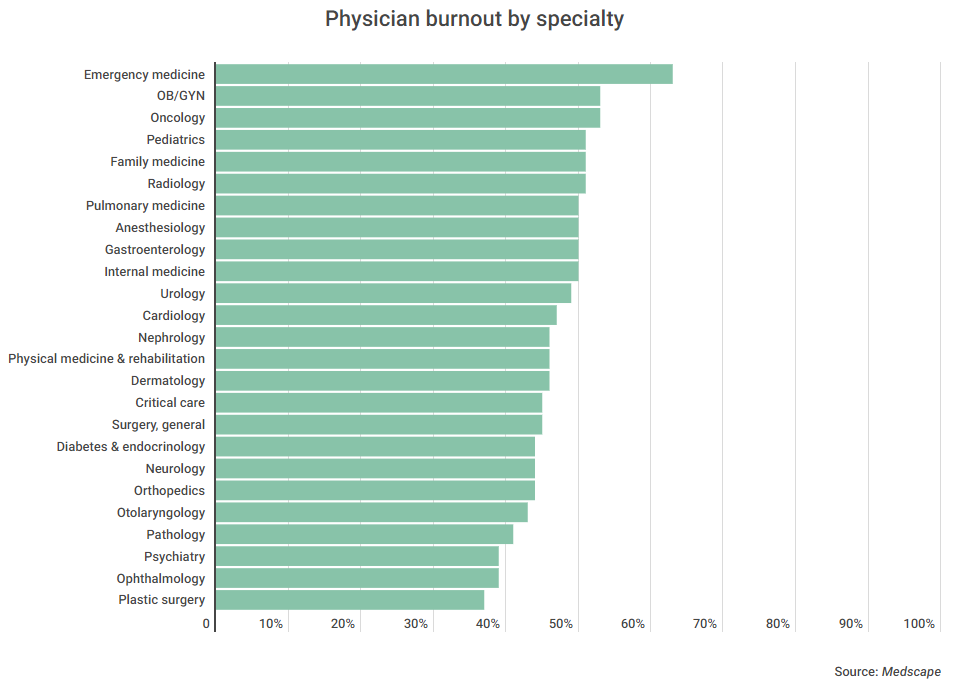
Below is Medscape’s chart on burnout by specialty. Given the COVID-19 pandemic, it’s unsurprising that ER doctors top the chart.
To deal with burnout, respondents reported using coping strategies like working out, spending time with family and friends, and sleeping more. But coping strategies won’t solve the underlying problem: business models that create and exacerbate high levels of provider burnout. Who can workout or take a walk when there simply isn’t time to do so?
Indeed, providers say that too many bureaucratic tasks, followed by too many hours at work, are the two largest contributors to burnout. According to Medscape’s study, reducing hours at work is the biggest lever providers have to reduce burnout. That seems logical.
If work is driving your burnout, and you want to be less burnt out, spend less time at work.
There is only so much that an individual can do from within the system. For example, if a provider elects to spend less time working, their depression and burnout will likely improve and their job satisfaction may increase. But their compensation will decrease, and they will be able to see fewer patients. Less provider burnout is good for the employer and patients, but it creates problems related to system-wide organization and planning. In this example, the employer is left to determine how to make up the workforce supply gap. A more effective approach to reducing hours at work and the associated burnout would be an organization-led movement and associated culture change.
At its root, physician burnout is a systemic problem, not a problem that should rest on any one individual’s shoulders. It costs our economy at least $4.6 billion per year. Because of its systemic nature, I’d argue we need a systemic solution. Therefore, the responsibility must shift to the businesses that employ providers. They must lead the course correction if we hope to maintain our current physician workforce.
Business model solutions that show promise at reducing burnout
So what systemic solutions are on the table? What would actually work? Below I dive into three of the most promising case studies:
Four-day work weeks/flexible schedules: In the corporate world, the four-day work week has gained a lot of attention. And we are now starting to see it infiltrate specific pockets of health care. For example, Mount Sinai was an early adopter of the four-day schedule for its nurse managers about two years ago. As reported by Becker’s, the change has improved nurse manager engagement and retention. There are also obvious benefits when it comes to recruiting.
Providence has also instituted a flexible work approach for its nurses, allowing them to work partially on-site and partially virtually. While they haven’t instituted a four-day work week across the board, they are focusing on flexibility and allowing nurses to make their own schedules. Instead of assuming everyone has to work a 12-hour shift, they’re also leveraging an AI tool to support four-, six-, eight-, and 12-hour shifts, without adding a lot of administrative burden. Similarly, Northwell also offers a shortened work week for some administrative and clinical roles.
Leveraging AI for charting: We need to alleviate bureaucratic tasks. In the last year, generative AI solutions’ have positioned themselves to help solve this problem..
The Advisory Board recently shared a case study on the University of Michigan Health-West’s implementation of Nuance’s Dragon Ambient eXperience (DAX) as an ambient charting solution to reduce physicians’ documentation needs and associated cognitive burdens. This DAX implementation resulted in lower rates of physician burnout, exhaustion, and disengagement for providers that used it over 60% of the time, per the study. Interestingly, the reduction in burnout was similar to the experience of a provider shifting from full-time to part-time work. If flexibility in work hours isn’t an option for organizations, ambient charting could be an alternative.
In Boston, at Brigham and Women’s hospital, some providers are using Abridge, another VC-backed ambient charting tool, to reduce time on bureaucratic tasks. ER physician and public health researcher, Dr. Jeremy Faust, recently talked about how this app, which “records and then converts the audio [of patient encounters] into well-organized, appropriately formatted medical notes for the electronic medical record” was an immediate “game changer.” He also pointed to the fact that it made his work both more enjoyable and easier. You can read his full write-up on this experience via Inside Medicine (note: it’s paywalled).
Ambient charting tools provide great promise in reducing physician burnout by alleviating administrative burden. But to drive impact at scale, they must in my opinion be embedded in the system’s strategy and business model.
Health system-specific initiatives: Before joining the Christensen Institute, I worked across innovation and corporate strategy teams at Atrium Health, now Advocate Health. One initiative I participated in during my time on the strategy team was “Best Place to Care.” This was an initiative led by the organization’s chief physician executive, Dr. Scott Rissmiller, to make Atrium Health the best place to provide care as a physician. A key focus of the work was to eliminate systemic barriers that inhibited doctors. I share this that case study here because it worked within a corporate setting. The initiative launched in 2019. When the pandemic hit, efforts doubled down to improve the working environment for providers, as opposed to going on pause.
The investment paid off for Atrium. Prior to the initiative, Atrium’s providers scored in the low 40th percentile of physician well-being. But a year after Best Place to Care changes were implemented, well-being rose above the 75th percentile. The AMA did a write up on this strategic initiative, which you can read more about here.
Why did this initiative succeed? Well, it was supported by the C-suite, it brought in mid-level leaders from across organizational functions to align on a mission, and it was grounded in an external review of the evidence. Simultaneously, leaders focused on hearing from physicians directly. It may seem obvious, but too often we fail to listen to providers to understand how organizations can support them. The result was improved physician well-being.
While these case studies are informative, it’s also important to look at larger scale studies.
What large-scale research says
Let’s look at some larger scale research on both six-hour work shift and four-day work week studies. You can probably guess how these initiatives went. Working fewer hours improved both worker health and productivity. One six-hour shift study from Sweden back in 2016 and 2017, involving nurses working in elder care homes, determined that nurses took less sick time, increased their productivity, and reported improved health.
In a four-day work week study out of the UK, which reported results at the start of 2023, 71% of employees reported reduced burnout. 39% said they experienced reduced stress, and 40% had fewer sleep issues. Notably, fatigue-related burnout costs companies around $2,000/employee/year. This figure may be even higher in health care where errors are more costly and sleep deprivation is culturally acceptable.
Over 90% of companies that implemented the four-day work week decided to keep it in place at the end of the study, though it’s unclear if any of these were health care entities.
What are the downsides of flexibility?
There are downsides to offering more workplace flexibility. The most obvious is the potential exacerbation of physician shortages, because of the limited hours clinicians would have available to see patients. As the population grows and ages, physician shortages are an increasingly large problem. According to the AAMC, 42% of practicing clinical physicians are over 55 years old, and 20% are over 65. The best solution here, of course, is to add more providers to the field.
A second downside is the operational challenge and cost of overhauling scheduling processes. There’s also a third: Reduced patient satisfaction. The scheduling issue may be easier to overcome, because of AI tools—but there are costs associated with any new technology investment. Health systems, hospitals, and practices would need to assess if the return on investment related to lower rates of provider burnout would offset these costs. Based on four-day work week studies and outcomes from nurse manager four-day week pilots, they might do so. However, each employer would need to evaluate the cost-effectiveness of such a change for their organization.
What’s the bottom line?
Health care may be conservative and slow-moving in many ways. But there’s evidence that a shorter work week, plus more flexibility, can work.
If shortened or flexible work weeks aren’t possible for a given organization, systemic changes that mimic the effects of one should be explored. Alternatively, there are alternative changes that could have a similar impact. Ambient charting tools are a decent place to start.
The key is organization-led flexibility that matches workforce desires and life commitments (such as parenting, caregiving for elderly parents, enjoying time in leisure and community, etc.). This organizational flexibility is required because burnout isn’t rooted in an individual’s inability to cope. It’s the result of ingrained business models that don’t support provider well-being. To fix the problem, we must address the root cause. And therefore, leaders need to take a hard look at their culture and organizational processes in order to drive change.
This was the first column as part of our new Second Opinion author series. If you’d like to apply to be an author, reach out at [email protected] with some specific topic ideas and writing samples.